





A country grappling with cardiac disease is a sitting duck for an anti-cholesterol drug that some say is a silver bullet to stave off heart attack even as others bash it for severe side effects, one of which includes encouraging cancer


A combination of poor dietary choices, fascination for junk food, a sedentary lifestyle and the stress of everyday life is making Indians highly susceptible to heart disease, say experts. Pics/Getty Images
When, at the beginning of this month, it was reported that a new study had found that statins, class of drugs, could help reduce the risk of fatality from breast cancer by 40 per cent (see box: The Beijing research), it was another potential trophy on the mantle for statins, which many cardiologists would happily call the wonder drug of this century.
ADVERTISEMENT
Statins are a class of drugs that block the enzyme in the liver called HMG-CoA reductase, which is responsible for making low-density lipoprotein i.e. LDL or 'bad' cholesterol in the body. LDL is known to cause plaque formation in the arteries, a medical condition called atherosclerosis, which can eventually lead to a heart attack, one of the leading causes of death across the globe.
According to the Medical Certification of Cause of Death report, in 2014, diseases of pulmonary circulation and other forms of heart diseases were the major cause of death with 1,40,000 deaths being reported in India. Of these 35,000 deaths were reported in Maharashtra. It's no wonder then that statins, which has left aspirin behind in the race, are now becoming both, the primary (preventive) and secondary (treating) drug for coronary artery disease in this country. Yet, as half the world praises statins, there are voices that advice restraint and raise questions whether the benefits of the drug (if any at all) outweigh the harm.
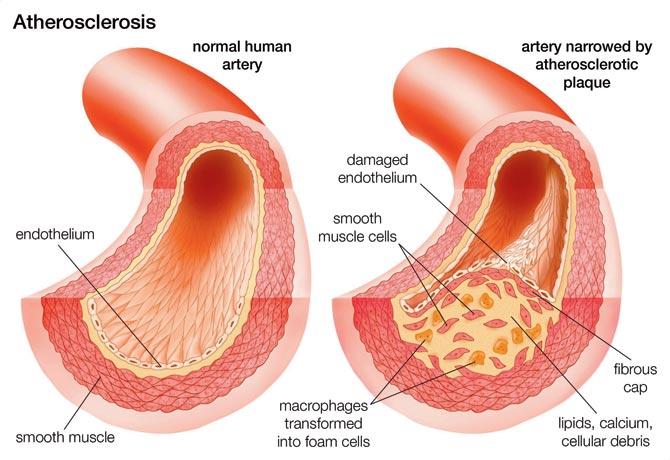
Atherosclerosis: Comparison of a normal artery with an artery narrowed by atherosclerotic plaque. (Photo By Encyclopaedia Britannica/UIG Via Getty Images)
The cholesterol conundrum
There's no ambiguity in Swedish independent researcher Uffe Ravnskov's designation. He is the spokesman of THINCS, The International Network of Cholesterol Skeptics, and has published several papers that question whether lowering the body's LDL levels - the primary occupation of statins - is beneficial.

Uffe Ravnskov’s, spokesman, THINCS
In a telephonic interview to mid-day, Ravnskov (MD, PhD), spoke about a research that he, along with 16 others, had conducted and published in the British Medical Journal (BMJ) in May 2016, titled, Lack of an association or an inverse association between low-density-lipoprotein cholesterol and mortality in the elderly: a systematic review.
"It was a review of 19 studies where the authors had followed a total of 68,094 people above the age of 60, for several years after they started taking cholesterol medicine. A few of them were on statins. When analysed how many of them had died, it showed up that those with the highest level of LDL cholesterol lived the longest. They even lived longer than those on statin treatment. Those with the lowest levels lived the shortest. That study totally disrupted the cholesterol hypothesis, because if those with the highest value lived the longest, why lower it? It's a relevant question as more than 90 per cent of those who die from heart disease have passed the age of 60."
In another study, Ravnskov says he analysed the association between cholesterol in the blood and the degree of plaque formation. "We found no association. Those with low cholesterol were just as susceptible as those with high cholesterol. We need to stop this cholesterol campaign immediately."
In fact, it is now argued that LDL is not bad for the body, and the body actually needs LDL to build its immune system. The paper by Ravnskov goes on to say that low LDL-C increases susceptibility to fatal diseases. "Support for this hypothesis is provided by animal and laboratory experiments from more than a dozen research groups, which have shown that LDL binds to and inactivates a broad range of microorganisms and their toxic products. Diseases caused or aggravated by microorganisms may therefore occur more often in people with low cholesterol, as observed in many studies."
Quoting another study in which one lakh healthy individuals were followed for 15 years, the paper said that "those whose initial cholesterol level was lowest at the start had been hospitalised significantly more often because of an infectious disease that occurred later during the 15-year follow-up period."
The relationship with cancer
While a certain amount of research says that evidence has shown statins to help prevent or cure cancer, several researchers claim the opposite. For instance, the authors of the paper say: "Another explanation for an inverse association between LDL-C and mortality is that high cholesterol, and therefore high LDL-C, may protect against cancer. The reason may be that many cancer types are caused by viruses… Furthermore, cholesterol lowering experiments on rodents have resulted in cancer, and in several case-control studies of patients with cancer and controls matched for age and sex, significantly more patients with cancer have been on cholesterol-lowering treatment."
Mark R Goldstein, MD and Fellow of the American College of Physicians (FACP), argues that treating cholesterol in cancer patients with statins could aggravate the disease. "Statins are immunosuppressive. This property might be beneficial in stabilising plaque in arteries. But, it might be detrimental if someone has cancer cells, since the immune system helps keep them in a dormant state."
"In one study we noted that on close analysis some cholesterol lowering trials suggested that there might be an increase in cancer in the group randomised to take statin therapy," he said of a 2008 article published by Current Oncology titled, Do statins prevent or promote cancer?
That statins are usually prescribed to the elderly, and might be most harmful to them is a worry for Goldstein.
Over prescribed or underused?
While the jury may still be out on the equation between statins and cancer, what is not debated is that the medication has a host of side-effects - muscle pain and damage, liver and kidney damage, increased blood sugar or Type 2 diabetes and in some cases, neurological side effects. What has been debated, however, is the severity of the side-effects and percentage of population effected.

Dr Vinod Kaneria, cardiologist, Khar’s Hinduja Healthcare Surgical
Cause of skeletal muscle pain
"The most common side-effect of statins is myalgia or skeletal muscle pain, and this occurs in 10 to 30 per cent of the people. What we call severe myopathy, i.e. where muscles are severely damaged, occur in about 0.1 per cent of the cases," said cardiologist Dr Vinod Kaneria from Khar's Hinduja Healthcare Surgical. In fact, as someone who treats patients of heart disease, Kaneria, who has been practicing for the last 25 years, argues that statins are under-prescribed in a country prone to the ailment.
"Now, we recommend that not just those above the age of 55 but even say, 35-year-olds who harbour risk factors like poor lifestyle and genetic history of heart disease, should take statins. The safety profile of statins have been proven through various trials and it works as a preventive drug," he added. However, a GP who has been practicing for over three decades, not wishing to be identified for this story, tells mid-day that the drug is being over-prescribed. "This is wrong. Today, most persons with diabetes are being prescribed statins. The doctors aren't checking the lipid profile. Only if cholesterol levels are haywire should statins be prescribed, and certainly not as a preventive measure. A drop in cholesterol levels is also a problem. In fact, HDL is a bigger culprit than LDL. Moreover, ultimately, it's the LDL-HDL ratio that is more important. It should be between 3 and 5."
He agrees with Goldstein that it's largely the elderly who are prescribed statins. "The aged are already battling weak muscles. Add to that the use of statins and the severe muscle pain is intractable and no painkiller works. When we stop the tablets, the pain disappears," he said.
Ravnskov said that independent researchers have shown that side-effects are very common, especially muscular problems. "Two trials were conducted. In one, 20 per cent suffered severe side effects while in the other, the number was almost 60 per cent."

Probing the mismatch
Last year, in an editorial for the British Medical Journal (BMJ), the publication's editor Fiona Godlee, called for an independent review of statins. Speaking to mid-day, she says, "There was a study published in Lancet last year with data collected a while ago, which said that there was no evidence of increased muscular pain. Another study said that there is no real evidence of benefits of statins. So, you are asking someone to take a pill for the next 30 years, without any seeming benefits."
 Fiona Godlee, British Medical Journal editor
Fiona Godlee, British Medical Journal editor
The bigger problem, she pointed out, is that the studies themselves haven't followed patients for 30 years. "So, we don't know the long term side-effects of the drugs, even if people are willing to take them. All I would say is that it's a live debate, one we should be having and independent research must continue."
Last year, BMJ had raised a red flag regarding the lack of data forthcoming from the drug companies (which sponsored the trials) and the triallists in statin researches. "My argument is that it's not just statins - it's a problem with other drugs as well - but that statins are so widely used. Why hasn't there been independent scrutiny? How many people of different age groups were there in the trial? How many of those belonged to low risk groups? How many women? This information should be in the public domain as the public is going to be taking the pill," said Godlee.
The statin trials, most of them sponsored by drug companies themselves, have been criticised. Requests for independent trials have not been met.

Dr Kamal Mahawar, consultant general and bariatric surgeon
Dr Kamal Mahawar, consultant general and bariatric surgeon at UK's Sunderland Royal Hospital, and author of The Ethical Doctor, said, "The drug companies are under no obligation to show results of the trials that show negative results. We are not getting the full picture, only the data that they want to see. This is a problem across the medical publishing world. If you are not seeing the full picture then you can be skewed in your analysis."
Prescribing with caution
Dr Krutarth Thakar, an oncologist at Wockhardt Hospitals, said that taking into account that statins theoretically suppress host T cell function and can promote carcinogenesis, especially in patients who already have poor T cell immune response, it should be used with caution especially while treating patients whose immune system has been compromised, such as those with HIV, those being treated for cancers, children or elderly, patients who have been treated for cancer in the past and patients with a strong family history of cancer.
Dr Kaneria has another point to make. In the 1990s, he says, he was part of a trial for Simvastatin (the first variety of statin to be introduced in India) at Nair Hospital, a subject he was interested in since his mother is a cardiac patient. In the West, he says, the average dose is of 40-80 mg. "In India, however, I have found patients doing well with 10-20 mg." Statins also react to a host of other medication and patients and doctors must be cautious. "A non-diabetic patient, taking Rosuva statin, has a nine per cent chance of developing diabetes mellitus. Also, it's not recommended to those above 80 years or more. Atorvastatin is considered safer in that age group, and then in a lower dosage, of say 5 mg."
Who decides what pill you take?
India, said Dr Mahawar, needs a body like UK's NICE i.e. National Institute For Health and Clinical Excellence. "It's the job of NICE to synthesise information for the general medical community and issue guidelines regarding medication and surgery practises; a body that is respected by general public and the media is needed here. We have no such body in India. There are societies of experts in a particular field. But they will issue guidelines that favour that field."
The Beijing research
Researchers from the National Cancer Centre in Beijing found that a common type of statin called lipophilic showed a particularly strong protective effect in breast cancer patients, compared with hydrophilic statins, which had a much weaker effect. Led by Dr Binliang Liu, from the department of medical oncology, the team examined seven existing studies covering 1,97,048 women and found that the use of any statins reduced risk of death from breast cancer by 27 per cent, and death from any cause by 28 per cent. The strongest effect on breast cancer was for women who were followed up for less than four years, where death from breast cancer was cut by 38 per cent. For women with more than four years of follow-up, statins did not appear to have any significant effect on death. One possible explanation for this could be that statins may simply be good at delaying death from breast cancer, or they may help prevent death from the types of breast cancer that kill people early. The research was presented at the American Society of Clinical Oncology (Asco) meeting in Chicago.
7.78%
The percentage of Indians receiving statin prescription in 2010, according to a paper by Choudhry NK titled, 'Despite increased use and sales of statins in India, per capita prescription rates remain far below high-income countries'. The paper says that little is known about statin use in lower-income countries. India is of interest because of its burden of cardiovascular disease, the unique nature of its prescription drug market, and the growing globalization of drug sales. "We conducted an observational study using IMS Health data for the period February 2006-January 2010. During the period, monthly statin prescriptions increased from 45.8 to 84.1 per 1,000 patients with coronary heart disease - an increase of 0.80 prescriptions per month. The proportion of the Indian population receiving a defined daily statin dose increased from 3.35 per cent to 7.78 per cent". The paper observes that only a fraction of those eligible for a statin appeared to receive the therapy, even though there were 259 distinct statin products available in January 2010. The low rates were accorded to access to healthcare, afforda-bility and underdiagnosis.
1987 The year the first statin, i.e. lovastatin, entered the market after being approved by America's Federal Drug Agency
6M The number of people in the UK estimated to be on statins
9% Chance that patients on Rosuva statin have of developing diabetes
 Subscribe today by clicking the link and stay updated with the latest news!" Click here!
Subscribe today by clicking the link and stay updated with the latest news!" Click here!
